

Kim Grajcar of West Palm Beach holds a photo of her daughter Samantha, who died of a heroin overdose. Bruce R. Bennett/Palm Beach Post/ZUMA
Each year, more than 40,000 Americans die from drug overdoses. That’s on par with the annual death toll from HIV/AIDS at the peak of the US epidemic, in the late ’80s and early ’90s, and far more than are killed each year from car accidents or gun violence. More than half of those overdose deaths involved opioids, a class of drugs including heroin, Vicodin, OxyContin, and fentanyl.
So dire is the epidemic of opioid addiction that it inspired a rare moment of political bipartisanship earlier this year, when Congress passed the Comprehensive Addiction and Recovery Act to increase accessibility to addiction medications and the overdose reversal drug naloxone. Democrats tried to include $920 million in treatment funding, but Republicans blocked the move, saying they would address the issue during the appropriations process this fall.
So what exactly is at stake? Here’s a quick primer on the scope of the epidemic—and what it will take to fix it:
What are opioids?
Opioids are compounds that bind to the brain’s opioid receptors, blocking pain and slowing breathing. Because the drugs trigger the release of the neurotransmitter dopamine, new users typically feel a calm, happy high. When users take opioids regularly, they develop a tolerance to the drugs, requiring more and more to achieve the same effect. In high quantities, the drugs reduce or stop breathing altogether, making overdoses often fatal.
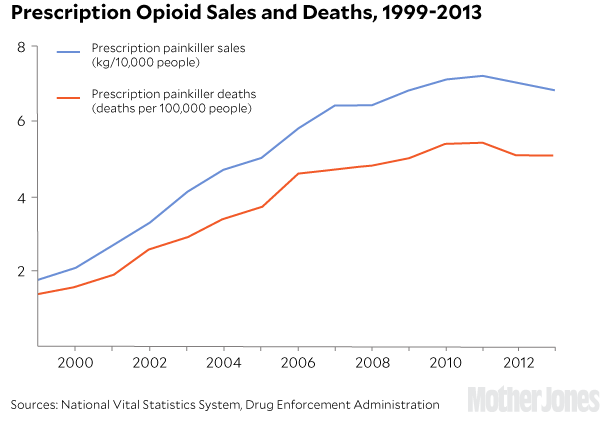
Some opioids, like heroin, are illicit; others, like hydrocodone or oxycodone (known by brand names Vicodin and OxyContin, respectively), are prescribed for pain relief but make their way to the black market. Prescriptions for the drugs have skyrocketed over the years, from 76 million in 1991 to nearly 259 million in 2012—enough to supply each American adult with “a bottle of pills and then some,” US Surgeon General Vivek Murthy has said. As of 2013, hydrocodone, the generic version of Vicodin, was prescribed to more Medicare patients than any other drug.
In an effort to curb the rampant drug abuse, the Drug Enforcement Administration reclassified some painkillers into a more restrictive drug schedule in 2014. Patients now need a written prescription from a recent doctor’s visit in order to pick up the drugs at a pharmacy. This spring, the Centers for Disease Control and Prevention released national standards urging doctors to limit the use of opioid painkillers for chronic pain. Effects of these efforts appear to be mixed: Deaths involving prescription painkillers have slowed, but overdose data suggests that some prescription drug users switched to heroin—a cheaper and often more potent option.
Now, authorities are scrambling to figure out how to address an influx of fentanyl, a painkiller up to 50 times more powerful than heroin. The drug, prescribed for acute pain but often produced illegally and mixed with (or sold as) heroin, has caused hundreds of overdoses this year, including Prince’s death in April, prompting investigations by the Centers for Disease Control and Prevention and the Drug Enforcement Administration. “For the cartels, it’s their drug of choice,” said Massachusetts Attorney General Maura Healey to the New York Times. “They have figured out a way to make fentanyl more cheaply and easily than heroin and are manufacturing it at a record pace.”
Why now?
Experts trace today’s epidemic back to the ’90s, when doctors started treating pain more aggressively. Physicians were taught that pain was the “Fifth Vital Sign” to be measured on a 10-point scale. Accrediting bodies began rating hospitals and physicians on how well they treated pain. “That’s when we started treating chronic pain the same way we treated acute pain—with short-acting narcotics,” says Kim Johnson, the director of the Center for Substance Abuse Treatment at the Substance Abuse and Mental Health Services Administration (SAMHSA). “It was kind of a perfect storm.”
Fueling the storm were pharmaceutical companies, which aggressively—and, in many cases, misleadingly—marketed painkillers to doctors and patients. Purdue Pharma, which introduced OxyContin in 1995, funded more than 20,000 pain-related educational programs between 1996 and 2002, according to an article last year in the Annual Review of Public Health.
Noting that doctors were wary of prescribing opioids because of concerns about addiction, the company funded studies finding that “physical dependence” on opioids is different from addiction and “clinically unimportant.” It provided financial backing to the American Pain Society, which introduced the “Pain is the Fifth Vital Sign” campaign, and the Joint Commission, which accredits health care organizations, in addition to other physician and patient groups. Purdue Pharma and its executives were fined more than $600 million in 2007 after they were found guilty of misleading regulators, doctors, and patients about the drug’s addictive qualities.
By 2010, the United States was consuming about 80 percent of the world’s opioid supply and 99 percent of the hydrocodone supply.
Who’s overdosing?
The overdose population stands out for being overwhelmingly white. That may help explain why, as we’ll get to below, this drug epidemic is often framed as a public health crisis rather than a crime wave requiring harsh punishment.
Unlike the heroin epidemic of the ’60s and the crack epidemic of the ’80s, both of which ravaged inner cities, heroin and opioid painkillers today are used at similar rates in rural and urban areas. Johnson, the SAMHSA Center for Substance Abuse Treatment director, attributes this partly to access: Like alcohol, you don’t need to get to a city to have plentiful access to prescription drugs. As the map below shows, many of the states hit hardest by the epidemic—like West Virginia, New Hampshire, New Mexico, and Ohio—are overwhelmingly rural and white.
Conventional wisdom holds that overprescribing is fueling the epidemic: Someone injures himself, is prescribed painkillers, and quietly develops an addiction. But that’s not the whole story: According to federal data, most people start out by taking the painkillers of a friend or family member. The best predictor of prescription opioid abuse is a history of other drug abuse, according to a recent study in Addictive Behaviors. Experimentation typically starts during adolescence or young adulthood.
How do users recover?
If an opioid user wants to stop using, there are two options: abstinence or medication-assisted treatment (also called maintenance treatment). Abstinence programs (often 12-step programs similar to Alcoholics Anonymous) have abysmal success rates when it comes to opioid addiction, with roughly 90 percent of program participants relapsing. Users who have gone through abstinence programs are twice as likely to overdose as those in medication-assisted treatment.
That’s why the scientific community, from the Substance Abuse and Mental Health Services Administration to the National Institute on Drug Abuse to the White House Office of National Drug Control Policy, support medication-assisted treatment—even if it’s indefinite and in some cases lifelong. When it comes to medication, there’s methadone, which has been around for decades but requires daily visits to a methadone clinic for observed dosing. And then there’s buprenorphine, a newer drug that many see as the gold standard. Like methadone, buprenorphine takes away cravings for painkillers or heroin. Unlike methadone, you can’t get high off of it, making it much harder to abuse. Ideally, after an initial dose adjustment period, it can be picked up at the pharmacy and taken like any other drug.
The biggest problem, both with methadone and buprenorphine, is accessibility: More than half of those who need treatment for opioid abuse don’t get it, according to Johnson. Patients routinely have to wait for weeks or months before a spot opens up in a program. 90 percent of US counties qualify as “methadone clinic shortage areas,” according to the RAND Corporation. Many patients don’t know about buprenorphine or can’t find a doctor to prescribe it. “Every time someone dies, I wonder, did they try to get treatment and not find it?”
What are politicians doing?
While Congress debates funding for the newly passed Comprehensive Addiction and Recovery Act (CARA), many states have taken matters into their own hands. Since 2001, at least 42 states have passed laws making naloxone available beyond hospitals, according to Pew Charitable Trusts. At least 31 states have adopted Good Samaritan laws, which give legal immunity to the bystander or friend who calls 911 to report an overdose. More than 3,000 drug courts have emerged since 1990, offering supervised rehab and periodic drug testing as an alternative to prison time. (It’s worth noting that drug courts are far from perfect; about half of them didn’t allow medication-based treatments as of last year. CARA aims to change that.)
The response by state and federal authorities alike—treating the epidemic as a public health crisis requiring expanded treatment access and reformative drug courts—stands in stark contrast with the responses to the harsh sentences called for in response to the crack epidemic. This may be partly because we’ve learned over the years that the war-on-drugs tactics don’t work, but it’s hard to ignore the race element: Opioids are killing white people.
The response “follows patterns we’ve seen over decades of drug scares,” said Marc Mauer, the director of the Sentencing Project, to the Marshall Project last year. “When the perception of the user population is primarily people of color, then the response is to demonize and punish. When it’s white, then we search for answers.”











