Brian Cassella/Chicago Tribune/Tribune News Service/Getty
All but three US states have very high or high levels of Covid-19 in their sewage right now, according to the CDC. Due to a drop in efforts to count individual cases, that data is the most accurate way to paint a picture of the current extent of Covid cases—and it’s bad.
In addition to wearing respirators, getting the updated Covid vaccine (mRNA shots were approved last week, and the Novavax vaccine this week) is an important way to reduce one’s chance of getting the infectious disease. Even if a person contracts it, the shot will reduce their risk of death and developing Long Covid.
But for uninsured and underinsured Americans, the vaccine has just gotten significantly more costly. On August 22, the CDC sunsetted its Bridge Access Program, which provided free Covid vaccines to 1.5 million Americans over the past year. A CDC spokesperson told Mother Jones that the sunsetting was a consequence of the new 2024-2025 vaccines being approved—which meant the 2023-2024 vaccines could no longer be administered. But many people did not know that the program would only cover the vaccine approved last year—just that it would end in August, potentially after the new shots became available. The CDC’s page on the program, which was live until some point Friday, did not clarify any of this information.
“For every step that you add in the process of trying to get a vaccine, you’re going to lose people.”
A rhetorical staple of the Biden administration is that it’s ensured people have the tools to fight Covid—but that is not the case for peopleunable to afford the updated vaccine out-of-pocket, which typically costs around $200.
Elizabeth Jacobs, an epidemiologist and professor emeritus at the University of Arizona, has studied the reasons why people do not get Covid-19 boosters. One reason, Jacobs says, is the logistics and challenges of getting the vaccines.
“For every step that you add in the process of trying to get a vaccine, you’re going to lose people,” Jacobs said.
Even before the end of the Bridge Access Program, getting vaccines has not always been easy. One person who spoke to Mother Jones said that he had to explain how the Bridge Program worked to pharmacists before he could get vaccinated for free.
The CDC, however, did announce that it has allocated $62 million for state and local health departments to buy vaccines for uninsured and underinsured people. However, the current surge and delays in implementation means people may fall by the wayside.
“I do have faith that $62 million will be used well to provide vaccines,” says Emory University epidemiology professor Jodie Guest. “Unfortunately, we just don’t have the details for how that will be done yet.”
Guest also notes that the up-front cost of subsidized vaccines is less of a burden on the healthcare system than a spike in the number of people severely ill with Covid. It is hard to know just how many people are currently hospitalized with Covid complications, as hospitals have not been required to report cases to the federal government since May. But the requirement to report respiratory viruses in hospitals will resume on November 1.
Since early in the pandemic, research has highlighted the risks of severe illness that low-income people, who are more likely to have chronic health conditions, face with Covid. These risks remain, and while it’s important that people with Medicare and Medicaid will be able to get updated vaccines, so should low-income people without health insurance.
“Vaccines are only as good as how vaccinated our immediate communities are.”
Children whose guardians are uninsured and underinsured will still be able to get vaccinated for free through the Vaccines for Children program, initially established by Congress in 1993 to make sure more kids were being vaccinated against measles. Chrissie Juliano, the executive director of the Big Cities Health Coalition, says that the ending of the Bridge Access Program underscores the “need for a permanent Vaccines for Adults program.” The Biden administration has proposed funding a Vaccines for Adults program in its proposed budget for the next fiscal year, but Congress could still reject it. In the meantime, Guest also recommends that people search for coupons at pharmacies that could bring down out-of-pocket costs.
“Vaccines are only as good as how vaccinated our immediate communities are,” Juliano said. “Vaccines protect us when we individually get it, but we really depend on our neighbors, our family, our friends [and] our classmates to also be fully vaccinated.”
While Covid-19 vaccines can reduce transmission, they are not perfect yet, which highlights the importance of wearing N95 and KN95 masks during surges, especially in medical settings, while traveling, and in other crowded indoor settings.
Jacobs finds it frustrating that masking is no longer promoted by public health agencies as it has become further politicized. “It is an established fact that respirators or high-quality masks reduce your risk significantly of becoming infected,” Jacobs said.
Given how many people the president sees and interacts with, it might be surprising that he hasn’t had Covid more often. The difference: this is the first major Covid wave where people around the president are no longer regularly testing. From his inauguration through March of this year, anyone visiting Biden at the White House had to test for Covid-19. Then the administration ended that practice—and Biden promptly got it again, a cautionary tale that drives home wider government failures to set public health ahead of getting “back to normal.”
Ten months earlier, in May 2023, the Biden administration ended the Covid-19 public health emergency, claiming that Covid “no longer meaningfully disrupts the way we live our lives.” That’s easier to say when everyone around you has to regularly test for the disease. Many people do not have ready access to Covid tests, and messaging from the US government that the pandemic is “over” doesn’t encourage people to get tested, nor to wear masks. Biden’s reluctance to mask publicly in recent months, even after ending regular tests for visitors, is the most visible—and important—example.
But Biden has the ability to dial back campaigning and isolate, working a limited schedule remotely. That privilege is not afforded to many other Americans, especially the blue-collar workers the administration claims to champion—who may not be able to pay their bills if they take time off. Ample rest reduces the risk of developing Long Covid; with workers being pressured to return to their jobs prior to five days—what the CDC previously recommended when someone is symptomatic—their risk of developing a long-term chronic illness increases, and the risk of losing their jobs with it.
Around 17 million adults in the US have Long Covid, according to KFF. For many, it’s a serious medical condition—the kind Biden has said could make him consider dropping out of the race. If he did, he would still have better treatment options than almost anyone else—another factor that might shape his risk tolerance.
There are many Americans who take Covid-19 seriously and encourage other people to do the same. Most do not have the same luxury of first-rate medical care, and anti-mask legislation like that in North Carolina can also lead them to be the target of harassment.
Later this year, Biden will get his updated Covid-19 booster. But again, many Americans will not be able to, as the program providing free Covid vaccines and boosters is sunsetting. Biden’s pandemic just isn’t the same as that of millions of working-class, low-income and disabled people. The weeks following his recovery, and the remainder of his term, are a chance to set a different example—both in his own pandemic safety choices and his administration’s.
One helpful characteristic of Covid, if there is such a thing, is that those who become infected shed the virus through their poop. Over the last few years, public health officials capitalized on this fact, and built a system to track Covid levels across the country using our sewage. Now, nearly four years after the start of the pandemic, as rates in many states swing upward yet again, the Centers for Disease Control and Prevention has released a helpful new tool for visualizing those trends.
With the agency’s Covid wastewater dashboard, users can chart historic, national Covid trends, identify which variants are on the rise, and view the states where “viral activity levels” are highest, meaning there may be an increased risk of infection. (Today, for instance, the levels are particularly high in the Midwest.)
New wastewater dashboard from the CDC! With national and regional trends at last! This is huge ⬇️⬇️ https://t.co/w4cd4D3yiP
As I’ve reported, the CDC’s National Wastewater Surveillance System, or NWSS, has been around since September 2020. But as CDC advisor Niall Brennan put it, the government’s first wastewater data visualizations were “underwhelming to say the least.” In putting the new dashboard together, he wrote on X, the CDC “willingly ripped up the rule book” to make the charts “more accessible to a wider audience.”
Well-understood wastewater data, however, isn’t just for curious nerds. It can also save lives. In March, I visited Houston, Texas—home to one of the country’s most effective wastewater surveillance systems—to see how their local wastewater tracking efforts worked. Here’s a bit of my dispatch from the trip:
[W]hat I found most compelling about Houston’s program is how city officials have used its sewer data to fight the virus. For one, explains Dr. David Persse, the city’s chief medical officer, it’s allowed hospitals to know when to expect a surge in patients, and when to avoid scheduling elective surgeries that would otherwise limit capacity. The city also conducts “pinpoint testing” at sewers just outside of schools, jails, homeless shelters, and assisted living facilities. (This requires a two-person team to physically visit each location and in some cases hoist sampling devices from cockroachey manholes.) Particularly in the early days of Covid, this site-specific testing served as a warning system: If the virus appeared in a nursing home’s wastewater, Persse says, “[we’d] test everybody, all the employees, residents—bada bing,we found it. And then they could control it.” According to Persse, just 8.4 percent of Covid deaths in Houston have been related to long-term care facilities, compared to an estimated 23 percent nationally.
Similarly, at a national level, wastewater surveillance “can be an early indicator that the number of people with COVID-19 in a community is increasing or decreasing,” according to the CDC. As I wrote this summer, it’s a bit like checking the weather, but for Covid. But unlike other types of COVID-19 surveillance methods, like collecting nasal swabs, “wastewater surveillance does not depend on people having access to healthcare, people seeking healthcare when sick, or availability of COVID-19 testing.” And the primary resource it does depend on—poop—is pretty darn reliable.
Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases, speaks during a press briefing at the White House, Tuesday, Nov. 22, 2022, in Washington. (AP Photo/Patrick Semansky)Patrick Semansky/ Associated Press
After nearly forty years as the nation’s top infectious disease expert, Dr. Anthony Fauci on Tuesday made what is likely his final appearance in the White House briefing room before he steps down from his positions as the director of the National Institute of Allergy and Infectious Diseases and chief medical officer to President Joe Biden. His departing message to the public: get vaccinated before the holidays.
“My final message, maybe the final message I give you from this podium, is, please, for your own safety and the safety of your own family, please get your updated COVID-19 shot as soon as you’re eligible,” Fauci told reporters.
The remarks come as families around the country prepare to gather for the holidays amid rising cases of various respiratory illnesses, including Covid. Last month saw a record number of hospitalizations for the flu. As my colleague Kiera Butler recently reported, hospitalizations for RSV in children have also skyrocketed.
“Every day for all of those years, I’ve given it everything that I have,” Fauci continued while reflecting on his leadership during the pandemic and beyond. His exit next month will mark the end of decades of public service, during which he oversaw the government’s response to two pandemics: AIDS and Covid. As I’ve previously written:
Before COVID, Fauci was most famous for his handling of HIV/AIDS. As the crisis began, he was harshly critiqued for not adequately marshaling the powers of the federal government to combat the disease under Reagan. ACT UP founder Larry Kramer wrote in 1988 that Fauci’s inaction made him a “murderer.” Since then, Fauci was won back over some activists by chipping away at HIV/AIDS. Peter Staley—who worked alongside Kramer with ACT UP—told us in an interview Fauci was “one of the great heroes in the fight against HIV/AIDS.”
But Fauci’s name is sure to continue living rent-free in Republicans’ minds. After spending most of the pandemic attacking Fauci, the GOP is set to make good on their threats to investigate him.
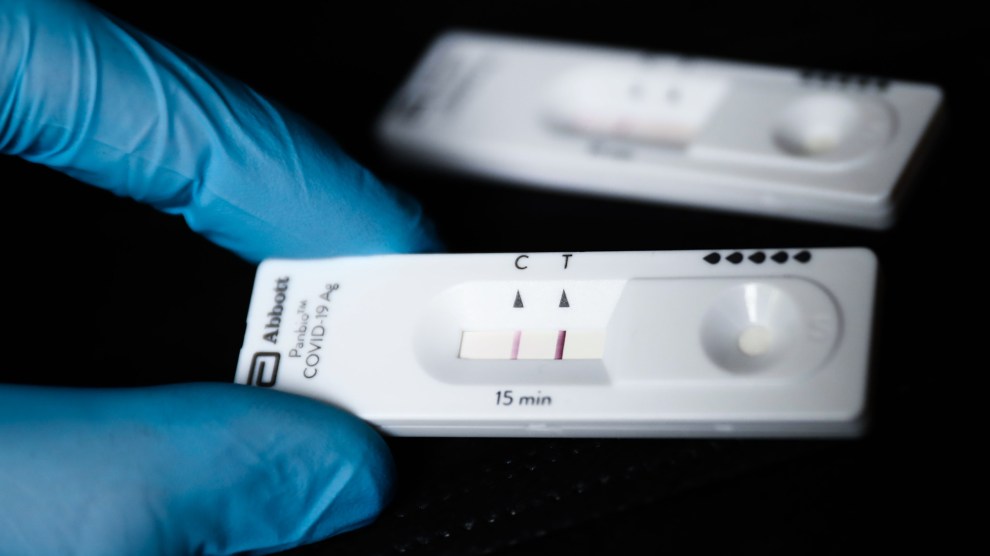
Rapid antigen tests Jakub Porzycki/NurPhoto via Getty Images
A friendly PSA: If you haven’t yet ordered your free at-home Covid tests through the US Postal Service, you’ve only got a few more days to get that done.
“Ordering through this program will be suspended on Friday, September 2, because Congress hasn’t provided additional funding to replenish the nation’s stockpile of tests,” federal officials have announced on the government’s Covid test website.
Each household is eligible for 16 rapid antigen tests through the USPS website, up from four free tests when the program launched earlier this year. After September 2, it will still be possible to get the tests covered through health insurance, whether directly or with a reimbursement.
In the spring, the Biden administration hoped to receive $10 billion from Congress to continue funding the pandemic response, but a deal for the funding did not succeed. As a result, Dr. Ashish Jha, the White House’s Covid response coordinator, said earlier in August that federal officials needed to stop spending so much money on tests and instead allocate resources for new vaccine booster shots that are designed to protect against the BA.4 and BA.5 coronavirus variants circulating around the country.
Those vaccines are expected to be available in September. They are “coming very, very soon,” Jha said at an event sponsored by the US Chamber of Commerce Foundation, according to CNN. He urged people to get the shot once they’re eligible. “These are substantial upgrades in our vaccines in terms of their ability to prevent infection to prevent transmission…[A]ll the data suggests it should be highly effective against the new variants.”
According to available data, Covid cases are now falling in the United States after surging this summer, but BA.4 and BA.5 remain widespread and are highly contagious. Jha noted that hospitals could come under strain this fall and winter because the flu season will kick in alongside another potential surge in Covid cases, particularly after states have continued to relax masking restrictions. “Under normal non-pandemic times, flu really stretches our health care system,” he said. “Throwing Covid on top of that, our health care system is going to get into serious trouble unless we are very proactive about preventing it, if we do nothing and just sort of hope for the best.”
The Omicron variant of Covid-19, which has overwhelmed hospitals and set new pandemic case records, is starting to wane in states that saw late surges—a sign that the worst of the highly contagious variant wave may have passed in the United States.
The latest available numbers reveal that Omicron is following a pattern from rapid acceleration to quick drop-off. In South Africa, where the variant was first identified, infections are down 87 percent from a mid-December peak. In the US, Omicron first hit the northeast. According to New York Timesdata, infections in those states started coming down as quickly as they rose—though new infection rates remain above last winter’s record. Now, the Times reports, rates are finally falling in the last states where Omicron surged:
The bad news is that hospitals remain overwhelmed. Since Covid-related hospitalizations and deaths lag behind infection rates, the pain this wave will inflict is probably at least a few weeks from dissipating. When it finally ends, the question will be whether there’s a new variant—and just how bad it might be. One contender nicknamed “stealth omicron” has already popped up in Europe. The future remains as uncertain as ever.
A worker dons a Grinch mask while waiting to help to direct travellers in the terminal of Denver International Airport Friday, Dec. 24, 2021, in Denver. More than 200 flights were cancelled by carriers out of Denver International because COVID-19 issues have created a shortage of workers. David Zalubowski/AP Photo
Last week, the Omicron variant of the novel coronavirus swept across the United States just as millions of people were preparing to visit family for the holidays. The spike in Covid infections hit the airline industry hard, causing employees to call in sick at high rates during the busiest time of the year. Predictably enough, a cascade of flights had to be canceled, leaving tens of thousands of passengers stranded in airports.
“Airlines canceled hundreds more flights Sunday, citing staffing problems tied to Covid-19, as the nation’s travel woes extended beyond Christmas, with no clear indication when normal schedules would resume,” the Associated Press reported Sunday afternoon.
Omicron is also hammering hospitals. As the New York Times reported Christmas Day, “[H]ospitals in Ohio running low on beds and staff recently took out a full-page newspaper advertisement pleading with unvaccinated Americans to finally get the shot. It read, simply: ‘Help.'”
The situation there is dire. The state “now has the country’s highest rate of Covid-19 hospitalization, and doctors say emergency rooms and I.C.U.s are running out of beds,” the Times notes. “They are being forced to call people in from holiday vacations as growing breakthrough infections whittle away at their staff levels.“
And other regions of the country are moving in the wrong direction as well, with surges reported in Arkansas, California, Delaware, Florida, Missouri, New Jersey, New York, and more.
The newest new Covid wave comes at a time when efforts to fully vaccinate the nation have stalled, hitting a wall of anti-vaccine sentiment. More than 39 million American adults—15 percent of the adult population— remain unvaccinated, and a recent Kaiser poll found that 87 percent of unvaccinated Americans say the new variant won’t spur them to get the jab. It’s unvaccinated people who are causing the spike in hospitalizations.
But stubborn US anti-vaxxers aren’t the only obstacle to a return to normal. In much of the globe, vaccines are still largely unavailable. “About 73 percent of shots that have gone into arms worldwide have been administered in high- and upper-middle-income countries,” the New York Times’ global vaccine tracker web page reports. “Only 0.9 percent of doses have been administered in low-income countries.”
The global anti-poverty charity Oxfam recently calculated that “more doses of Covid-19 vaccines have been delivered to the EU, the UK, and the US in the six-week run-up to Christmas than African countries have received all year.” With more than 40 percent of the world’s population unvaccinated, the virus has ample opportunity to mutate and generate an entire Greek alphabet of variants that can spread globally, ruining very much more than just Christmas travel.
The Biden administration announced a new set of measures Tuesday for tackling the Omicron variant, which has rapidly become the most dominant coronavirus variant in the United States.
President Biden’s plan involves setting up new federal testing sites, sending 1,000 military medical professionals to overburdened hospitals, and buying and distributing 500 million free rapid tests to the public. The new plan is a significant step up from the actions that the Biden administration announced it would take to combat the coronavirus three weeks ago. That plan promised that private insurers would reimburse consumers for the cost of rapid at-home COVID tests—starting January 15.
At a press conference this afternoon, Biden acknowledged that the Omicron variant increases the risk of breakthrough infections, but also stressed the importance of vaccinations and booster shots to reduce the severity of any potential illness. “A case of COVID-19 for a fully vaccinated and boosted person will most likely mean no symptoms or mild ones similar to the common respiratory viruses,” he said. “Over 200 million Americans share the peace of mind that they did not have in March 2020. They’re protected from hospitalization and are protected from death.”
This article has been updated with details from Biden’s afternoon press conference.
For the last week, every passing day in New York has felt a little more ominous. Upstate counties are facing overwhelmed hospitals, and Covid-19 cases are surging in the city, even among the fully vaccinated, due in part to the new Omicron variant. Lines for PCR testing in my neighborhood stretch for blocks, and response times for those test results seem to be lagging. Restaurants shut their doors. Parties were canceled. The Brooklyn Nets were so desperate for healthy players they reactivated the vax-less Kyrie Irving—who was promptly forced to quarantine. And now we have the numbers to show for it: On Friday, New York state posted its highest recorded number of positive Covid-19 tests since the pandemic began.
There are a few big caveats to that number. The first is that in the Spring of 2020, when New York City was the epicenter of the global pandemic, testing was so limited it almost felt like a scandal that an entire NBA team could get them—so there’s no comparison with that moment. The second, of course, is that most of the adult population is vaccinated, and a significant number of people have gotten booster shots, and they seem to have a good deal of protection against the variant’s worst effects. This isn’t March of 2020, no matter how ominous the tick-tick-tick of canceled sporting events and disrupted travel plans might be.
But it still sucks. It’s been almost two years of this. It’s the holidays! Everyone’s traveling and people are trying to catch up on the cheer they missed last year. And even while many aspects of the pandemic are greatly improved—we have better treatment options, and vaccines, and understandings of how it spreads, and lots of masks, and tests—there are still familiar hang-ups. Tests are embarrassingly expensive (in the UK they’ll send you tests for free), and the Biden administration—which once mocked the notion of sending out free tests—has rolled out a Rube Goldberg-ish process to curb costs. Per the New York Times:
The administration has said that it plans to issue its rules for reimbursement by Jan. 15, and the plan will go into effect sometime after that.
The administration has already said that the plan will not provide retroactive reimbursement for tests that have already been purchased, which means that any tests you buy for the holidays will not be covered.
January 15th!?
Stay safe, everyone. Get tested before you travel. And get that booster yesterday.
An art installation no the National Mall commemorating all Americans who have died of COVID-19 on September 24, 2021. Yasin Ozturk/Anadolu Agency/Getty
When the United States hit 100,000 COVID-19 deaths in May of 2020, it was a pretty big deal. The New York Timesmourned the “incalculable loss” in a full page headline. Even Donald Trump grudgingly acknowledged the toll.
On Sunday, with far less fanfare, the US hit 800,000 COVID deaths, according to a Reuters tally. That appalling milestone comes with deaths and cases again rising amid cold weather and continued vaccine refusal, and with the highly transmissible Omicron variant poised to contribute to the surge.
Eight hundred thousand is roughly the same as the number of Rwandans estimated to have been killed in the 1994 genocide there. It’s more than the population of North Dakota. Worldwide, meanwhile, COVID has killed at least 5.3 million people, according to a New York Times estimate. The real number is probably much higher.
Official COVID deaths, those that hospitals or coroners say were caused by the virus, will pass one million next year, maybe in the spring at current rates. But public health experts argue that COVID’s actual toll has already reached that grim milestone. Measures of excess mortality, a measurement of deaths from all causes above the number public health experts expected, jumped in many US communities as COVID surged. These measures suggest the actual death toll is about 20 percent higher than the official tally. Some of those added deaths aren’t from COVID—they could be people who failed to get medical treatment due to hospitals being overwhelmed. But these are real losses linked to the pandemic.
And the deaths are concentrated among people of color. They surged “in place like Albuquerque, New Mexico; Miami-Dade County, Florida; Jersey City, New Jersey; and New York City,” researchers from the Brown Institute for Media Innovation and MuckRock’s Documenting COVID-19 project wrote last week.
If you count those people, “the number of Americans who have died from the virus could be closer to 1 million,” the researchers wrote.
Deaths mount while the Republican Party makes resistance to vaccine mandates a key plank ahead of what are expected to be big gains in the 2022 midterm elections. On December 8, every Senate Republican, along with two Democrats, voted to overturn President Joe Biden’s proposed mandate for large private companies to require workers to either get vaccinated or to undergo regular COVID testing.
Around 60 million adults older than 12 in the US remain unvaccinated. Those people face a far greater risk of serious illness or death from the disease. A Texas study found last month that unvaccinated people are 13 times more likely to get COVID and 40 times more likely to die of it compared to those who are vaccinated.
In July, after President Joe Biden said coronavirus misinformation on Facebook was “killing people,” an anonymous company official jawed back, saying Facebook would “not be distracted by accusations which aren’t supported by the facts.”
But behind the scenes, Facebook employees were already beginning to reckon with a flood of false anti-vaccine claims on the platform. According to a company memo obtained by the Wall Street Journaland released this morning, around the time COVID-19 vaccines became widely available last spring, “roughly 41% of comments on English-language vaccine-related posts risked discouraging vaccinations.” The document and other internal memos show, the Journal writes, “that Facebook has often made minimal or ineffectual efforts to address the issues and plays them down in public.”
Facebook’s efforts to crackdown on anti-vaccine content—like its laggard response to its role in spreading falsehoods and hate, including political disinformation and QAnon conspiracies—ran into several hurdles. Although CEO Mark Zuckerberg personally supported making the platform a haven for credible, public health information, users didn’t, and quickly flooded private Facebook Groups and the comments of major posts with misinformation.
Anti-vaccine content was twice as prevalent in comment sections as in posts, one memo found, but the company’s ability to detect and take down problematic comments was “bad in English, and basically non-existent elsewhere,” a Facebook data scientist wrote in one memo. The company’s systems didn’t always make it easy to remove or demote posts. After Facebook employees singled out a viral post that claimed vaccines “are all experimental & you are in the experiment,” it remained up because “Facebook’s systems mistakenly thought it was written in Romanian.”
While Facebook’s role in spreading vaccine-related misinformation has been a topic of public discussion throughout the pandemic, even as internal researchers identified the problem, the company avoided public acknowledgment and generally remained defensive. Guy Rosen, Facebook’s vice president of integrity, argued in a July blog post that “vaccine acceptance among Facebook users in the US has increased.” Responding directly to Biden’s criticism of the company, Rosen said, “The data shows that 85% of Facebook users in the US have been or want to be vaccinated against COVID-19. President Biden’s goal was for 70% of Americans to be vaccinated by July 4. Facebook is not the reason this goal was missed.”
But internally, the Journal reported, “Facebook documents show it had been playing catch-up for months, trying to manage the flood of misleading and false information aimed at undermining the vaccine effort.” Upcoming congressional hearings could bring further revelations; as the Journal points out, “Facebook officials have become concerned that Mr. Zuckerberg or Chief Operating Officer Sheryl Sandberg may face questions from lawmakers about how their past public statements on these issues square with the company’s internal assessments.”
Medical staff move COVID-19 patient who died onto a gurney to hand off to a funeral home van, at the Willis-Knighton Medical Center in Shreveport, La., Wednesday, Aug. 18, 2021. Gerald Herbert/AP
Just three months ago, the United States averaged fewer than 25,000 COVID infections a day, with an average of 627 COVID deaths over a seven-day period. It was the end of May and it seemed as if the light at the end of the proverbial COVID tunnel was near just as the “hot vax summer” was about to begin.
Then, as more and more Americans became vaccinated, too many—to the tune of 47 percent of Americans as of Sunday—have refused. And among that group of people, the more transmissible Delta variant spread like wildfire. Now, at summer’s end, as the nation averages more than 160,000 infections per day, more than 100,000 daily hospitalizations, and more than 1,500 deaths, the highest rates since March, epidemiologists, public health officials, and, frankly, many Americans are asking: When will this end?
In places where vaccinations are low, the wave of infections has pushed hospitals to the brink of a crisis. In Mississippi, just 38 percent of residents are fully vaccinated, and the surge in cases and hospitalizations, particularly among children, have strained hospitals. At the University of Mississippi Medical Center, the state’s only level one trauma center, the emergency room and ICU are beyond capacity, with exhausted hospital workers treating patients in a “logjam” of beds scattered in the hallways and in triage rooms. During a recent news conference, Dr. LouAnn Woodward, the head of that medical center, said, “We, as a state, as a collective, have failed to respond in a unified way to a common threat.”
In Florida, where Republican Gov. Ron DeSantis has been aggressively antagonistic toward mask mandates and measures that would curtail COVID’s spread, the state is seeing its deadliest period in the pandemic, averaging 244 deaths per day, higher than its peak last summer. Just 44 percent of residents are vaccinated in nearby South Carolina where the state is averaging 5,400 new COVID cases per day, the highest infection rate in the country. Steve Benjamin, Democratic mayor of Columbia, the state’s capital, announced he planned essentially to defy the Republican governor’s ban of mask mandates by imposing a local state of emergency and order students to wear masks if COVID cases keep rising.
I’m an optimist.
I always have been.
But everyday South Carolinians are being devastated by poor leadership & decisions.
What’s more, the CDC recently found that unvaccinated people are 29 times more likely to be hospitalized from COVID than those who are vaccinated, further burdening hospital resources. Part of the issue, of course, is that only kids 12 years and older can currently get vaccinated, and the reopening of schools for in-person learning has amplified concerns over the spread among children, teachers, and their families. CDC research found that between mid-June and late August, COVID hospitalizations rose fivefold among children and teenagers.
But the story of unvaccinated versus vaccinated children could be considered a microcosm of the unfolding of the pandemic generally. Even though children under age 12 cannot be vaccinated, Dr. Anthony Fauci, the nation’s top infectious disease expert, recently said that they likely won’t begin to be until “hopefully by the mid, late fall and early winter.” But for those who can get vaccinated, it’s clear that the shots work to curtail hospitalizations. The rate of COVID hospitalizations was 10 times higher among unvaccinated children compared to vaccinated ones. And tellingly, pediatric hospitalizations were roughly four times higher in states with the lowest vaccination rates than in those with the highest, further showing that vaccines curtail severe disease even among children.
What does this all mean? It means we’re in the midst of yet another period of uncertainty that’s likely to continue if we fail to vaccinate enough people and take actions such as mask mandates to curb the virus spread. A Washington Post/ABC News poll showed that 52 percent of Americans supported vaccine mandates from businesses and two-thirds of those polled supported school districts requiring mask wearing for students, teachers, and staff. Even so, that same poll found that even though they are more concerned than in June, more than 60 percent of unvaccinated Americans saw “low” to “no” risk of contracting COVID.
“People are pretty burned out 18 months into this thing,” Ezekiel Emanuel, professor of medical ethics and health policy at the University of Pennsylvania, told the Washington Post. “And the exhaustion has been made worse by the rapid seesaw we’re having—take your masks off, put them back on. It’s all very confusing, but we have to be honest: We don’t know when, we don’t know how. We don’t know.”
As the school year starts for millions of children across the country, coronavirus cases among kids are on the rise. The American Academy of Pediatrics is reporting that between August 5 and August 26, 500,000 children tested positive for COVID-19—a five-fold increase since July. The alarming rise in cases comes as many students are returning to in-person classrooms and conservative parents protests against mask and vaccine mandates designed to keep kids safe.
Despite the rollout of the vaccine, the Delta variant of the coronavirus is surging across the country, particularly in states where vaccine rates remain low. The vast majority of the people getting infected, hospitalized, and dying from the virus are the unvaccinated—which includes children under 12 who are not yet eligible for the vaccine. Because the youngest among us cannot be inoculated, we have to rely on other measures to keep them safe, like masking, distancing, testing, and ventilation.
The consequences of ignoring public health restrictions are grim. More than 220 children’s hospitals are pleading with the Biden administration for help as the increasing number of child patients are straining the staff and their facilities. “Our children’s health care safety net is under unprecedented strain,” Children’s Hospital Association CEO Mark Wietecha said in a press release. “Children’s hospitals and their dedicated staffs are doing their part, and we hope every American, the White House and Congress can help.”
Unfortunately, not everyone is concerned about the safety of children. An alarming number of parents have tried to interfere with public health protocols at schools. On Thursday, an Arizona elementary school called a parent of a child at the school to inform him that his child had been exposed to the coronavirus and needed to quarantine at home. The child’s father, instead, showed up to the school with two other men and zip ties.
When they arrived, according to the Washington Post, they told school staff that they were there to arrest the principal. “If you insist on this, I’ll have you arrested,” one of the unidentified men said. “We’re ready to make a citizen’s arrest if necessary.” The principal informed the men that he was simply following guidance from the county health department and called the police. The men left before law enforcement arrived.
A health care worker draws up a dose of the Moderna COVID-19 vaccine in Novato, California.David Paul Morris/Bloomberg/Getty
As the Delta variant spreads across the country, and breakthrough cases among vaccinated people are on the rise, health officials in the United States are rolling out plans for booster shots—even as much of the world waits for their chance at the first shot.
The Biden administration announced that boosters should be available to those who have received the Pfizer or Moderna vaccine as soon as September 20. Studies are underway to determine the importance of supplemental doses for those who received Johnson & Johnson, with experts thinking boosters for the single-dose shot will likely be needed, too. Which means that more than 5 million Americans—with priority given to health care workers, nursing home residents, and elderly adults—might be eligible to receive third shots later next month, and even more Americans are soon to follow after that. Already, in Israel, extra doses are available to many immunocompromised individuals as well as people over 50; Germany, France, and the UK have begun to make plans to offer boosters this fall.
As wealthier nations race to roll out boosters, many global health experts have cautioned against the rush. Only 1.3 percent of people in low-income countries have received at least one dose.
Administering boosters in the US while much of the world cannot access vaccines isn’t just ethically dubious. Experts say this could drag the pandemic on even longer, especially while Delta and other variants continue to travel. As long as vaccination rates are low in other parts of the world, more robust variants will continue to crop up.
It’s possible that some of these evolutionarily fit viruses could evolve to escape immunity acquired through prior infection or vaccines. Biden’s former chief COVID-19 adviser, Andy Slavitt, explained it well in this thread:
COVID Update: The debate on whether Americans should be offered 3rd shots as boosters in not a simple one.
Some experts say the boosters could delay the pandemic by at least another year:
Predictable, somewhat understandable & 100% will prolong global pandemic another year. Our struggle is not getting protected individuals more protected as we have no indication it will lower case rates. Our struggle is vaccinating unprotected individuals so they do not die https://t.co/LX80SgR7GY
Earlier this month, WHO Director General, Tedros Adhanom Ghebreyesus called for a global moratorium on vaccine boosters at least until September. On Monday he cautioned that “vaccine injustice and vaccine nationalism” in wealthier countries will allow more time for variants to mutate and spread. The organization’s Africa director, Matshidiso Moeti, blasted wealthy countries that have begun administering extra shots, saying the decision “makes a mockery of vaccine equity.”
While #COVID19 vaccine shipments seem to be taking off, Africa is encountering headwinds. Moves by some countries to introduce booster shots threaten the promise of a brighter tomorrow for Africa.
As some richer countries hoard vaccines, they make a mockery of vaccine equity. pic.twitter.com/fk4ChXFCye
Michael Ryan, the emergencies chief at the WHO, added that “we’re planning to hand out extra life jackets to people who already have life jackets while we’re leaving other people to drown.”
Pitting boosters against global equity is simply a “false choice,” said White House Press Secretary Jen Psaki. She noted that the US has donated more than 110 million vaccines to other countries.
What’s more important might be that five days after the initial announcement about pursuing boosters, the White House released data that showed that protection from vaccines against symptomatic infection wanes after six months. With that information available, some experts have argued, it would have been hard for the Biden administration not to justify boosters for Americans.
Even before Biden announced that the US will begin administering boosters, many Americans were taking extra inoculation into their own hands, often with a “mix and match” approach, despite WHO’s advice against making your own vaccine cocktail. The CDC reported that around 1.1 million people have already received unauthorized third doses of Pfizer or Modern vaccines.
But with a limited global supply of vaccines, Madhukar Pai, a global health researcher at McGill, said it really is a “zero-sum game.”
In many other countries, barely 1 million have been able to receive vaccines. In Cameroon, for example, a country with 26 million people, only a little over 395,000 have gotten vaccinated. Or take Bangladesh, one of the world’s most populous countries, where less than 10 percent of the population has gotten the jab.
“The most vulnerable everywhere in the world should be kept safe from COVID as soon as reasonably possible,” Jerome Singh, a professor of public health who specializes in ethics in global health at the University of Toronto told me.
Singh noted that previous policies, like the United States’ ban on exporting raw materials needed for vaccine production in April (which has since been lifted), had a “paralyzing impact” on vaccine availability worldwide.
“It’s ethically problematic to suggest that vulnerable people in the US should be prioritized for a third dose when equally vulnerable people in many low- and middle-income countries have yet to receive their first dose. The lives of vulnerable people everywhere have equal moral worth.”
People wait for a distribution of masks and food from the Rev. Al Sharpton in the Harlem neighborhood of New York. Bebeto Matthews/AP
During the COVID pandemic, life expectancy for Black Americans fell by 2.9 years. Latinx Americans, who typically live longer than Black Americans and whites, lost three years of their lives. Now, a new Centers for Disease Control and Prevention study published Friday found that Black, Latinx, and Native Americans/Alaskan Native adults have died at startlingly higher rates during the COVID pandemic than in typical years, illuminating the disparate suffering communities of color have faced in the last year and a half.
In the CDC’s Morbidity and Mortality Weekly Report, researchers looked at the excess mortality incidence rates, a wonky term that means the number of people who have died in a population above their community’s expected number of deaths. They assessed the number of excess deaths per 100,000 people across the US between December 2019 and January 2021 by race and age and observed changes in death trends over the course of the pandemic.
The researchers found that for adults older than 65 years old, Black Americans died at an excess rate of 1,033 per 100,000 people while Latinx adults died at an excess rate of 1,007 per 100,000—a far cry from white Americans, who died at an excess rate of 500.1 per 100,000. And for Black adults over 65 years old, 78.7 percent of excess deaths were directly attributed to COVID. For Latinx adults over 65, the percentage was 85 percent. And for white Americans over 65, that percentage stood at 93 percent.
As researchers zoomed in on younger adults, though, the disparities in excess death rates became starker. While white Americans between 25 years old and 64 died at an excess rate of 51.2 per 100,000, Latinx Americans died at nearly 99 per 100,000 and Black Americans died at a startling excess rate 133 per 100,000. What’s more, excess deaths among Alaskan Natives and Native American adults between 25 and 64 occurred at a staggering rate of 221 per 100,000.
This is a lot to digest. Let me share a graph with you.
The numbers are complicated, but the resulting message isn't. Researchers concluded that the findings could help "guide targeted public health messaging and mitigation efforts to reduce [COVID] disparities" and "highlight the importance of timely data to address inequities in social determinants of health that increase the risk for death from COVID-19 among racial/ethnic minority groups." The CDC study affirmed what Black, Latinx, and Native American/Alaskan Native communities have experienced since early 2020: Unprecedented death and despair, thanks in large part to a pandemic that has exposed just how unequal the country is.
Passengers wait in a long line to get a COVID-19 test to travel overseas at Fort Lauderdale-Hollywood International Airport. Marta Lavandier/AP
In recent weeks, hospitals across the country have felt overwhelmed with the surge of coronavirus cases. On Saturday, Florida reported nearly 24,000 new cases, an all-time single-day record for the state. Meanwhile, in the last seven days, Louisiana, at 693 cases per 100,000 people, has the highest number of new cases per capita in the United States, followed by Florida (627) and Arkansas (502). Dr. Joe Kanter, the state’s top health officer, told the Associated Press that 1 percent of Louisiana’s population contracted COVID-19 in the past two weeks.
Zoom out, and one can see an even more troubling trend: When compared to other countries with populations over 1 million people in the last seven days, Louisiana is tied with Botswana for the highest daily case average per capita in the world—at 99 cases per 100,000 people, according to the New York Times‘ coronavirus case tracker for the United States and the world. Florida, meanwhile, is not far behind with a daily average of 90 per 100,000 people, ahead of nearby Cuba (81 per 100,000). “If Louisiana and Florida were countries, and not states, Louisiana would be the highest incidence country in the world and Florida would be the fourth one,” epidemiologist Michael Osterholm said on MSNBC last week.
If Louisiana was a country, it would be #2 on Earth in COVID cases per capita this week to Fiji. Florida not far behind. pic.twitter.com/xzfd48w1JU
The troubling surge comes as GOP governors like Florida’s Ron DeSantis and Texas’s Greg Abbott have imposed statewide bans on mask mandates in schools as their states’ hospitals grapple with the surge in COVID cases. In Louisiana, where just 37 percent of people are fully vaccinated, Democratic Gov. John Bel Edwards has reissued a statewide mask mandate, even as his Republican attorney general undermined it.
But some Republican lawmakers have shifted gears as their states suffered from the Delta variant. On Sunday, more than three months after he signed a law barring local mask mandates, Arkansas Gov. Asa Hutchinson said on CBS’s Face the Nation that his decision was an “error,” adding: “Facts change, and leaders have to adjust to the new facts and the reality of what you have to deal with.” And Louisiana Republican Sen. Bill Cassidy, a physician who contracted COVID, told CNN’s Dana Bash on State of the Union that he disagreed with DeSantis’s ban, noting: “When it comes to local conditions, if my hospital is full and my vaccination rate is low and the infection rate is going crazy, we should allow local officials to make those decisions best for their community.”
The United States has returned to the grim milestone of 100,000 new coronavirus infections per day. As the highly transmissible Delta variant surges and vaccination rates remain low in some parts of the country, infection rates are returning to levels not seen since last winter, before vaccines were available.
Fifty percent of Americans are vaccinated and 70 percent of adults have at least received one dose of the vaccine. Children under 12 are still not eligible for the vaccine. But despite widely available vaccines, many states across the south, such as Florida and Tennessee, have dismal vaccine uptake, leaving their populations vulnerable to the new variant.
This latest surge comes right as the school year is set to begin. Adults refusing to get vaccinated combined with officials weary of imposing mask mandates at schools across the country has created a nightmare for parents, teachers, and students attempting to stay safe from the virus. DeSantis threatened to withhold funding from Broward County schools after the district tried to implement a mask mandate for the school year. In Tennessee, the state House Speaker Cameron Sexton threatened to call a special legislative session to provide vouchers for parents to change schools if any district shuts down or imposes a mask mandate. Meanwhile, the number of children infected with coronavirus is on the rise.
It’s not just new infections. The vaccines have so far proven to largely prevent serious illness and hospitalization, but the unvaccinated are causing a surge in hospitalizations too. The Southeast has seen a 50 percent increase in hospitalizations, leaving health care workers overworked and hospitals overrun. Florida, Georgia, Louisiana, and Mississippi account for 40 percent of hospitalizations—in those states doctors are worried about running out of beds and turning patients away eerily reminiscent of the early days of the pandemic. “We are seeing a surge like we’ve not seen before in terms of the patients coming,” Dr. Marc Napp, a Florida doctor told the Associated Press earlier this week. “It’s the sheer number coming in at the same time. There are only so many beds, so many doctors, only so many nurses.”
As the spread of the highly contagious Delta variant shatters coronavirus case records in Arkansas, its Republican governor is scrambling to reverse a ban on local mask mandates he signed into law just months ago. But as Gov. Asa Hutchinson admitted in a press conference Monday, rolling it back will be difficult—and something he probably can’t do without broader support from his party’s lawmakers.
“In hindsight, I wish that had not become law,” Hutchinson told reporters. “But it is the law and the only chance we have is either to amend it or for the courts to say it has an unconstitutional foundation.” The governor, who last week declared a public health emergency amid surging COVID cases, is now calling for a special legislative session to amend the ban. But Hutchinson’s admission of regret may not be enough to convince the state’s GOP-controlled legislature.
Resistance to vaccines has exacerbated the crisis, with Arkansas communities accounting for some of the country’s lowest vaccination rates. Last week, Hutchinson faced vaccine hesitancy firsthand when he was roundly booed on stage after challenging the lie that vaccines cause fertility issues.
While Hutchinson was just one of many GOP governors to enthusiastically embrace a ban on mask mandates earlier in the pandemic, he is the first to try to roll back such an order. His move stands in stark contrast to other Republican governors still doubling down on them, as in Florida, Mississippi, and Texas, even as their states see cases explode. As I wrote earlier:
On Saturday, Florida recorded 21,683 new cases of COVID-19, breaking its one-day record for new cases. But even as the state swells with fresh infections, Republican Gov. Ron DeSantis remains hellbent on his war against mask mandates. He even recently barred school districts from instituting mask mandates when classes reconvene in August.
DeSantis is far from alone in his bitter fight against mask-wearing, a measure health officials say is critical in the fight to contain the highly contagious Delta variant. In Mississippi, where ICU beds are nearing capacity with a surge of unvaccinated individuals, Republican Gov. Tate Reeves blasted the CDC’s mask guidelines as “foolish” and claimed that it reeked of “political panic.”
“It has nothing, let me say that again: It has nothing to do with rational science,” Reeves said on Thursday.
On Monday, President Biden directly called out Republican governors who are blocking schools and businesses in their states from instituting mask mandates, telling them to “get out of the way.”
“Some governors aren’t willing to do the right things to make this happen,” Biden told reporters. “I say to these governors, please help. If you aren’t going to help, at least get out of the way of the people who are trying to do the right thing. Use your power to save lives.”
The rollout of children’s COVID vaccines has begun: On Monday, the FDA approved the Pfizer shot for 12- to 15-year-olds. That’s just the beginning—last week, the New York Timesreported that children as young as 2 could be eligible as soon as September. The mass vaccination of children could herald the end of the most catastrophic social costs from the pandemic in the United States: Schools and day care facilities will be able to resume normal operations, which means parents will no longer have to perform the nearly impossible act of juggling simultaneous work demands and child care. Cue the collective sigh of parental relief: It’s the moment we’ve all been waiting for!
Well, maybe not all of us. According to an April poll by the Kaiser Family Foundation, nearly a quarter of parents surveyed said they definitely wouldn’t get their child vaccinated, and an additional 15 percent said they would only have their child vaccinated if their school required it. About a third said they didn’t plan to get their children vaccinated right away; instead they planned to wait and monitor for side effects.
In some ways, this was to be expected. The vaccines are new, and they were approved under an emergency-use authorization during a historic pandemic. Nathan Chomilo, a pediatrician in Minnesota and a spokesperson for the American Academy of Pediatrics, told me that parents of his patients have expressed very understandable concerns—that the trials seemed rushed, for instance (they weren’t), and questions about whether kids really need the vaccine, given their relative unlikelihood of severe COVID. (Most experts agree they do.) Chomilo notes the importance of language in describing what’s going on. “I’ve really tried to use the term ‘vaccine deliberation’ when it comes to the COVID-19 vaccine versus lumping it in with this broader, longer-term issue of ‘vaccine hesitancy,’” he said.
But where Chomilo sees a need for nuanced conversations, anti-vaccine advocates likely see a grand opportunity to broaden their base with a group of parents—people who may never have thought twice about keeping up with the standard schedule of vaccines for infants and children but now are questioning the safety of a new shot. Experts have observed an uptick in anti-vaccine organizing over the last year. Rupali Limaye, a Johns Hopkins public health researcher who studies vaccine hesitancy, told me via email that she is “worried about the growing following behind some prominent antivaxx groups.” She sees these forces not only as barriers to mass vaccination against COVID but also as direct threats to herself and her colleagues. She added, “There seems to be more coordination among those that have these attitudes, and this has led to coordinated attacks/take downs of public health officials.”
Even before the COVID vaccines were approved for teens, anti-vaccine groups were already out in force in online parenting communities. A few viral posts round up entries from the Vaccine Adverse Event Reporting System, the federal database where people can report any symptoms they’ve experienced after a vaccine. These posts are compelling—like this one from an anti-vaccine advocate purporting to find a pattern of heart problems in 16-year-olds who have received a COVID vaccine.
What the people behind the posts don’t disclose is that VAERS reports aren’t verified independently, nor are they official medical reports: Anyone can submit an entry. But this is a perfect template for how misinformation works: Its spreaders omit key context or details and hope readers will have an emotional reaction without thinking too hard about the veracity of what they’re reading.
That’s just one tactic, of course. Throughout the pandemic, I’ve reported on the proliferation of anti-vaccine sentiment in online parenting communities. I’ve examined how anti-vaxxers took over homeschool moms’ groups, and how coronavirus deniers and QAnon conspiracy theorists won over moms’ communities on social media. As the year wore on, I’ve noticed a few patterns of misinformation that are repeated in these groups, and I expect to see them crop up again during the rollout of vaccines for children. In the coming weeks, you’re likely to see posts designed to appeal to the Whole Foods shopper types (“Do you really know what’s in those vaccines?”), the anti-corporate types (“Big pharma’s making bank on these vaccines!”), and the Libertarians (“Don’t let the government tell you what to put in your kid’s body!”).
You’ll see more subtle posts, too, which will appeal to one’s sense of identity as a caring and vigilant parent. Are you the kind of parent who will unquestioningly do what you’re told? Or are you the more savvy kind who will rely on your own intuition about what’s best for your family? Aren’t you the kind of parent who will do your own research?
This last category of these posts may be the most important because psychologically it can be the most effective. The reasons that moms’ groups are particular targets of anti-vaxxers are complex, but there’s one dynamic that I think deserves more attention. I’m going to go on a little tangent here, but bear with me—I promise this is relevant to vaccines. A few weeks back, Katie J.M. Baker wrote in Lux about the proliferation of anti-trans sentiment in UK moms’ groups. Baker observed members seeing trans people who bore children as a threat to their burgeoning identity as moms, as if moms’ group members required exclusive ownership of the physicality of motherhood. Baker quotes one group member: “Carrying my child and birthing my child was not a fucking social construct.” She chronicles how this kind of outrage gets whipped up in the groups with trans people becoming the scapegoats.
Of course, Baker is writing about something entirely different, but vaccine misinformation can follow a similar pattern. In these groups, the physical acts of motherhood—like unmedicated childbirth and breastfeeding—are powerful markers of identity. These acts are often talked about as “superpowers.” Many mothers, and perhaps especially the ones who spend a lot of time in Facebook groups, can feel vulnerable, lonely, and overwhelmed. They may have scant family leave and little help at home. Sometimes, their real concerns about their own health and their babies’ wellbeing have been dismissed by doctors.
For years, purveyors of misinformation about alternative health have exploited these forums to promote theories and practices that aren’t backed by science and can be dangerous. Some of the greatest hits: Ultrasounds can harm your developing fetus; Tamiflu will kill your toddler; a mere sip of formula will destroy your infant’s microbiome; and you should eat your placenta to ward off postpartum depression. The unifying theme for all of them is that the savvy parent “does her own research” to guard against profiteering hospitals and pharma-aligned doctors. It’s not a big intellectual leap to get from that mindset to vaccine skepticism.
Much of this misinformation can be found interspersed with inspirational feel-good messages in the public Facebook group Natural Parenting Mommas. With 143,000 followers, the group lists among its subjects of interest attachment parenting, baby-wearing, holistic health, and natural birth methods. Typical posts range from TikTok videos defending the right to breastfeed in public to memes criticizing standard obstetric practices such as cervical exams. Many of the posts have a feminist vibe; there are countless memes about the thankless work of mothering. You can imagine readers murmuring tearfully, “I feel so seen!” “What men don’t understand is…nobody cooks for her,” reads one. “Nobody cleans for her. Nobody makes her meals. Nobody does her laundry. Nobody makes sure she’s okay. Nobody caters to her, period. A woman is always instantly looked at as someone who needs to take care of everyone.” Some of the memes that the group shares are full of cathartic anger about sexual violence. One recent post:
I wish men understood that when women are talking about feminism and rape culture and shit, it’s not just a political conversation. It’s not about being a “social justice warrior” or whatever. It’s about our actual lives being shaped by misogyny since childhood, and the daily reality of living in fear of violence. This isn’t a fucking game or philosophical debate. This is our fucking lives.
An overarching theme is the paramount importance of parenting. “Your job will forget you ever worked there,” reads one post. “Your child will never forget you weren’t there.”
Over the last year, though, ominous messages about public health during the pandemic have been woven into posts about the sanctity of motherhood. Recent posts warn members about the psychological damage that mask mandates will cause in children. “Protecting kids from dangerous things like forced masking, traumatizing isolation, toxic injections, harmful foods & oppressive government isn’t a #conspiracy theory, that’s just called good parenting,” one March post read. Another recent post is a message in a frame of brightly colored feathers reminiscent of a Native American dreamcatcher. It reads: “Your daily reminder: Don’t take the COVID vaccine.” (When asked about the group’s stance on COVID vaccines and mask mandates, a spokesperson for Natural Parenting Mommas wrote back, “Considering there are multiple admins for the page, all with varying degrees of opinions on the COVID vaccines and mask mandates, we will be unable to confirm anything for you at this moment in time.”)
Women come to moms’ groups for the reassuring memes about how hard and lonely parenting can be, and they stay for the righteous indignation about the government presuming that it knows what’s best for their families. “New parents are left alone, without meaningful conversations from trusted, credible sources,” Seema Yasmin, a Stanford physician who studies medical misinformation, told me this week. Many people are drawn into social media groups in the vulnerable postpartum period, when they’re just forming their identity as parents. That early influence is powerful, and it can persist for years. “That’s how you end up with people really deeply entrenched in a parenting groups on Facebook, with conspiracy theories about everything from ‘if you eat your placenta, you won’t get postpartum depression’ to ‘don’t vaccinate your kid.’”
The pressure on parents is even greater with the added burden of the coronavirus, said Jennifer Reich, a sociologist at the University of Colorado, Denver, who studies the anti-vaccine movement. “During the pandemic, as people have felt more isolated, online communities have become more important than ever,” she told me. “Parents in general and mothers specifically have relied on online communities for a long time for advice and support.”
Katy Strang, who moderates a Facebook moms’ groups in Camarillo, California, told me she has observed this dynamic in her own group. She and her fellow moderators try to remove posts that pass on unverified information, but as she told me last fall, during the pandemic, it’s become a nearly impossible task. When I caught up with her this week, she said the incredible strain of pandemic parenting has made the situation worse. “To our detriment,” she wrote me in an email, “the isolated, exhausted mamas who look to these groups for support at all hours of the days and nights may be susceptible to internalizing misinformation that is being shared by armchair experts.”
The slow cascade in online groups from alternative health to COVID misinformation is not easy to fix, especially since its very proliferation serves to normalize the content. It won’t go away if social media platforms simply label posts as misinformation. The moderators I’ve interviewed have told me that even their efforts to delete misinformation haven’t worked; the deleted posts just pop up in the comments section on seemingly unrelated posts. The fundamental reason these tactics won’t work is that they’re not addressing the right problem, which is not a lack of knowledge, but a lack of support.
There are some things that might actually counteract misinformation, and they have nothing to do with offering facts as an argument. Instead, programs such as paid family leave, affordable and accessible child care, and universal basic income for women who choose to remain home could be antidotes to all the alienation at the core of these groups. Yasmin notes that simply improving postpartum care and training doctors to take parents’ concerns seriously could also diminish the roles that online forums play in parents’ lives. “Historically, we’ve not done a great job of supporting new parents, especially when it comes to health areas that all are already stigmatized,” she said. “I worry that we’ll just lose many more people. And we will foster more distrust against the medical field.”
In the context of the pandemic, that distrust is intensified, and it’s evident in the spaces I report on. As the world gears up for children’s COVID vaccines, this will persist. You’ll hear people blaming online moms’ groups for being anti-science, for being hotbeds of misinformation. When you do, remember this: It’s not that the mothers are dumb or overly credulous—it’s that they’re desperate.
Researchers have long known that the coronavirus is airborne, lingering in floating particles that spread whenever an infected person coughs, sneezes, or simply exhales. It’s the reason public health authorities have been urging schools to improve ventilation as part of their reopening plans: Bringing in more clean outside air can dilute the virus in classrooms, hallways, and cafeterias, helping to prevent spread. But thousands of schools across the country have gone a step further, using high-tech air cleaning systems in an attempt to fight COVID-19—often paying for air purifiers with federal CARES Act money intended to make schools safer during the pandemic.
Now, a top seller of one of the most popular high-tech air purification technologies among schools is facing a federal class action lawsuit claiming that its devices could produce toxic chemicals in classroom air and do not work as advertised to fight COVID, according to a court filing.
“Global Plasma Solutions Inc. preys on people desperate to cleanse the air and protect themselves from ailments including the COVID-19 virus,” alleges the complaint filed in US District Court in Delaware on May 7. “Defendant’s ‘profits over people’ scheme won the company acclaim, publicity, and generated hundreds of millions of dollars in sales.”
Global Plasma Solutions (GPS) is one of the country’s top manufacturers of purifiers that use a technology called bipolar ionization: small machines, usually installed in air ducts, that zap passing air molecules and give them a positive or negative electrical charge. According to the company, those charged molecules, called ions, spread through the room, destroy pathogens, and eliminate other harmful contaminants. GPS claims its devices can eliminate 99.4 percent of the coronavirus from surfaces in 30 minutes and 98.3 percent of the coronavirus from the air in 60 minutes. Schools have found the pitch compelling: GPS says over 1,300 K-12 schools have installed its devices, and demand has only increased over the last year. The lawsuit, which was filed by Robert Garner, a Maryland resident who bought a GPS ionizer for $750.67 in March, estimates that GPS has sold “tens of thousands of units” at minimum.
The company’s claims about COVID are “deceptive,” overstating the purifiers’ ability to fight COVID and “instilling customers with a false sense of security through misleading claims,” according to the lawsuit. Testing that GPS touts as “independent” is actually paid for by the company itself and employs unrealistic experimental conditions, the complaint adds. It cites an investigation published last week by Kaiser Health News, which found that one of the company’s COVID tests amounted to blasting the virus with 27,000 ions per cubic centimeter in a chamber the size of a shoebox. (In a full-sized room, the complaint adds, the machine would generate a concentration of 13 times fewer ions.) A GPS spokesperson says that further tests in larger chambers, with lower ion concentrations, still reduced airborne coronavirus by more than 90 percent. While 2,000 ions per cubic centimeter is a “minimum goal,” she adds, some real world spaces using the company’s technology reach more than 40,000 ions per cubic centimeter.
All in all, the lawsuit paints a picture of an air purification company whose products make the air worse, not better. “Defendant’s misrepresentations and false statements were woven into an extensive and long-term advertising campaign,” the complaint says, citing company webpages and other marketing portraying the ionizers as safe and effective. “The misleading representations grew like a virus.”
Back in March, I interviewed Delphine Farmer, a chemist at Colorado State University who was at the time working with other scientists on one of the only peer-reviewed studies on bipolar ionization in real-life environments. Farmer warned about the unintended consequences of using what she described as an unproven technology:
As an environmental chemist, I think about the precautionary principle, where you say, “Well, if this might do harm, and you don’t need to do it, then you just shouldn’t use it.” You have to prove that something is benign—that it’s not going to hurt the environment, and it’s not going to hurt people before you use it. And I think this rush to market these air cleaning devices is very concerning. I think we’re creating devices that might—not guaranteed—but they might create some some dangerous byproducts. And they certainly haven’t been proven to be effective.
Farmer’s study, which was published in the journal Building and Environment later that month, tested GPS devices in an experimental chamber and an occupied office building. While the experimenters didn’t test for the coronavirus, they found the machines did little to remove particulate matter from the air and actually appeared to produce some concerning byproducts. The class-action lawsuit filed Friday argued that GPS machines are not as safe as the company’s advertising would make it seem, because the gaseous byproductsdetected by researchers included “harmful toxins including Acetone, Ethanol, Toluene, and Butyraldehyde.”
The study by Farmer and her collaborators had immediate consequences for communities struggling with how to safely open schools: During a school board meeting in Montclair, New Jersey, last month, it fueled questions from parents worried about the GPS ionizers recently installed in local schools. (According to the local newspaper, the district has decided to turn off the machines until they can be researched further.)
GPS, meanwhile, has gone on the offensive, publishing a rebuttal to the Building and Environment study and pointing to what the company says are flaws in the experimental design. Since March, GPS also filed defamation and product disparagement lawsuits against two indoor air engineering consultants who have publicly criticized the company’s products and testing, including one who likened the air purifiers to cigarettes. “We intend to aggressively defend our technology and claims,” a GPS spokesperson told me. “Testing in independent labs and feedback from thousands of installations demonstrate that GPS technology works, is safe and can play an important role in making comprehensive air cleaning and filtration systems even more effective. We will review the complaint and respond accordingly.”
A judge has yet to rule on whether the lawsuit, which claims more than $5 million in damages for consumers nationwide, can proceed as a class action. Yet it all but ensures that the question of whether GPS bipolar ionizers work—and whether they are dangerous—will be litigated in court, with potentially devastating results for GPS. After all, the company now finds itself standing in the same shoes once occupied by the Sharper Image, whose signature product (along with massage chairs) was an ionizing air purifier called the Ionic Breeze, which used an earlier version of the technology now employed by GPS’s devices. In 2005, a series of articles in Consumer Reports claimed that the Ionic Breeze did little to clean particulates from the air, but produced harmful byproducts—in this case, ozone. Like GPS, the Sharper Image fought back with a defamation and product disparagement lawsuit. It lost. And soon, like GPS, Sharper Image was facing a nationwide class action lawsuit that helped drive it into bankruptcy.
This story has been updated to provide more context about GPS’s coronavirus testing.
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we’re known for don’t happen under corporate ownership. We shine a bright light into the dark corners of power and report the facts other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you. Please stand with Mother Jones and make a donation today. These are dangerous times, and we’ve got a lot of hard, consequential work to do. But we can’t do it without reader support.
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we’re known for don’t happen under corporate ownership. We shine a bright light into the dark corners of power and report the facts other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you. Please stand with Mother Jones and make a donation today. These are dangerous times, and we’ve got a lot of hard, consequential work to do. But we can’t do it without reader support.