The American Medical Association’s new training on pain management arrived in the midst of a burgeoning crisis. It was September 2007, and doctors were prescribing enough opioid painkillers each year for every American adult to have a bottle of the addictive pills. Overdoses were at a historic high and showed no signs of slowing down. Just four months earlier, executives at Purdue Pharma had pleaded guilty to felony charges for misleading regulators and physicians about the dangers of OxyContin.
In light of this news, one might have expected the AMA—the prestigious organization that bills itself as the “unified voice” of America’s doctors dedicated to “the art and science of medicine and the betterment of public health”—to bring attention to the crisis in its newly updated continuing education course on how to treat pain.
Instead, the 12-module training suggested that doctors were still too tentative about prescribing narcotics. “The effectiveness of opioid therapy may be undermined by misconceptions about their risks, particularly risks associated with abuse and addiction,” read materials from one session. The class included ideas like “pseudoaddiction,” referring to when pain patients seem “inappropriately drug seeking,” but aren’t truly addicted—rather, they just needed more pills.
For young children who were unable to verbalize their pain, materials encouraged prescribers to use the “Poker Chip Tool”: lay out four poker chips in front of a child, explain that the chips are “pieces of hurt,” and ask how many pieces of hurt the child has. The course instructs, “Do not give children an option for zero hurt.”
Thousands of physicians took the course, which was first released in 2003 and updated periodically over the next decade. Recently, I asked Dr. Roneet Lev, chief medical officer to the Office of National Drug Control Policy from 2018 to 2020, to take a look at the modules. She concluded, “I would call this ‘How to Create an Addict’ education.”
Perhaps that shouldn’t come as a surprise: Down in the fine print, the AMA-branded course materials reveal that the training’s development and distribution was made possible by an educational grant from Purdue Pharma.
By now, the story of how Purdue Pharma sowed the seeds for the overdose crisis is the stuff of history books, HBO specials, and a dizzying number of lawsuits. The company paid patient advocacy groups, medical societies, and academic experts in an unprecedented marketing blitz for OxyContin, laying the foundation for the rampant opioid prescribing of the 2000s and 2010s and for today’s profusion of illicit opioids, like heroin and fentanyl.
But the years of Purdue’s involvement with the AMA have been strangely absent from that narrative. Between 2002 and 2018, the AMA and the organization’s philanthropic arm, the AMA Foundation, received more than $3 million from Purdue Pharma—ranking them among Purdue’s top-paid third-party groups, according to previously unreported court documents. While the AMA stopped receiving funding from Purdue in 2007, it continued to offer the Purdue-funded pain management course until at least 2014, and the AMA Foundation didn’t stop accepting donations from Purdue until 2018—well after the opioid crisis had morphed into a full-blown epidemic.
Purdue’s relationship with the AMA Foundation was particularly cozy: As Richard Sackler oversaw the meteoric growth of OxyContin as the president of Purdue, he also sat on the board of directors of the foundation, from 1998 until 2004. The foundation website at the time boasted that Sackler’s “familiarity with research, business and medicine” would help “support the medical community.” For years after Sackler’s tenure, Purdue was a “platinum level” foundation donor, a distinction shared in 2016 by just Purdue and Pfizer. The status earned Purdue’s executives spots at semiannual meetings with the upper echelons of AMA leadership, including the AMA’s chief executive and the chair of its Opioid Task Force.
Even if you’ve never heard of the AMA, it affects your life. The organization helps determine the content of your doctors’ medical school training and the continuing education they receive, sets the ethical conventions that they are expected to abide by, helps decide hospital safety standards, and plays a key role in determining the cost of medical services. Its representatives advise the public on all manner of health issues, from police brutality to the Delta variant. With $430 million in annual revenues, the AMA advocates on behalf of its 272,000 doctor and medical school student members and nearly 200 affiliated medical societies. It publishes the prestigious Journal of the American Medical Association, one of the most widely circulated general medical journals in the world. The AMA Foundation, with some $25 million in assets, funds medical school scholarships and community health initiatives. And over the past two decades, the AMA has been the third-largest spender on political lobbying, topped only by the US Chamber of Commerce and the National Association of Realtors.
“I can tell you from my own personal experience, [AMA] members really do move medicine,” then–Surgeon General Jerome Adams said during a talk at the group’s 2018 annual meeting. “AMA is who Congress listens to. The state medical societies and associations are who the state legislatures listen to.”
Again and again over the past decade, the AMA has used this political clout to push back against efforts by federal agencies to curb opioid prescribing. Its leaders have argued to federal regulators that there is “no bright line” when it comes to how big of a dose of opioids is too big, that putting limits on opioid prescribing takes “treatment decisions about pain care outside of the physician-patient relationship,” and that landmark guidelines drafted by the Centers for Disease Control and Prevention “lacked a patient-centered view.”
In 2018, when members of Congress were hesitant to back legislation that would, among other things, mandate that doctors receive training on addiction before prescribing opioids, Sen. Joe Manchin (D-W.Va.) reportedly summed up the problem: His colleagues were “too scared to take on the AMA.”
The AMA contends its behavior is driven by a primary principle: protecting the sacrosanct doctor-patient relationship. In emails to Mother Jones, the organization denies that its positions are influenced by donors, and claims that it has always advocated policies that are determined democratically by its legislative body. Indeed, there are plenty of physicians who are well versed in the history of the opioid crisis who still agree with the AMA’s foundational argument, that politicians shouldn’t be involved in patient care.
But critics have long argued that the organization uses its white-coated prestige as a veneer to advocate on behalf of the medical industry—whose interests are, at times, diametrically opposed to those of the public’s health. This criticism predates the opioid crisis: A 1994 New England Journal of Medicine study found that the AMA’s political action committee gave far more money to politicians who opposed the AMA’s purported stances on things like gun control, tobacco cessation, and abortion than those who supported them. The organization has also repeatedly led the charge against progressive attempts to provide universal health care, even while making big profits off public health systems. “The AMA may accomplish things that help patients, but make no mistake, it is a doctor-first organization…Protection of the power, privilege, and the pocketbooks of physicians is the AMA’s compass,” concluded journalists Howard Wolinsky and Tom Brune in their 1994 history of the association, The Serpent on the Staff.
“That is often a pharma line: ‘Patients are individuals, physicians need to be free to make their own decisions,’” says Dr. Adriane Fugh-Berman, a Georgetown University professor of pharmacology and physiology. “It’s always what they say when they’re advocating against the evidence.”

In the mid-’90s, the AMA’s stance on opioids echoed the prevailing notion in the medical field: namely, that the drugs are addictive. “For severe back pain your physician may prescribe a narcotic painkiller, such as codeine, hydrocodone, or propoxyphene,” reads a 1995 AMA Pocket Guide to Back Pain. “These drugs are usually prescribed only for short periods, however, because they are addictive and are not necessary for long-term pain control.”
By 2000, the AMA’s stance had flipped. That year, its Council on Scientific Affairs found that “addiction seems to occur infrequently” from opioids, and that “physicians’ fears of regulatory scrutiny play a part in the undertreatment of pain.” The organization contended that for many patients, opioids “are the most effective way to treat their pain, and often the only treatment option that provides significant relief.”
Many medical institutions and regulatory agencies reversed their position on opioids around this time. When Lev, the former ONDCP officer, was getting her start as an emergency room physician in San Diego in the ’90s, she recalls thinking it was odd that there was so much pressure—from senior physicians, from medical associations, from the state medical board—to treat pain with opioids. “When you’re a younger doctor, or that’s not your specific area of expertise, you tend to listen to senior people,” she says.
By the mid-2000s, Lev estimates, a fifth of patients in the ER were in withdrawal or looking for painkillers. “I would say, ‘I don’t think you need this, but here’s some Percocet,’” she remembers. “With good intentions, I was following the standard of practice.” Later, after she began meeting the parents of children who had overdosed on painkillers, she started to push back on opioid prescribing. Her colleagues suggested that she didn’t have enough compassion for patients in pain.
The rise in opioid prescriptions was largely fueled by Purdue’s historic launch of OxyContin in 1996, and, along with it, an unparalleled pharmaceutical marketing campaign. According to the previously unreported court documents, between 2002 and 2015, Purdue spent $115 million funding hundreds of third-party organizations, including patient advocacy groups, medical societies, and law enforcement associations. While the AMA and its foundation were among the top recipients, PhRMA, the powerful pharmaceutical lobbying group, was the biggest beneficiary of Purdue’s third-party spending, receiving a whopping $23 million over the 14-year stretch.
“Any marketing message that a pharmaceutical company can get into the voice of a third party is a more effective marketing message for them,” says Fugh-Berman. And when it comes to the AMA, she adds, “What a powerful organization to have as a third-party marketer. It’s this behemoth.”
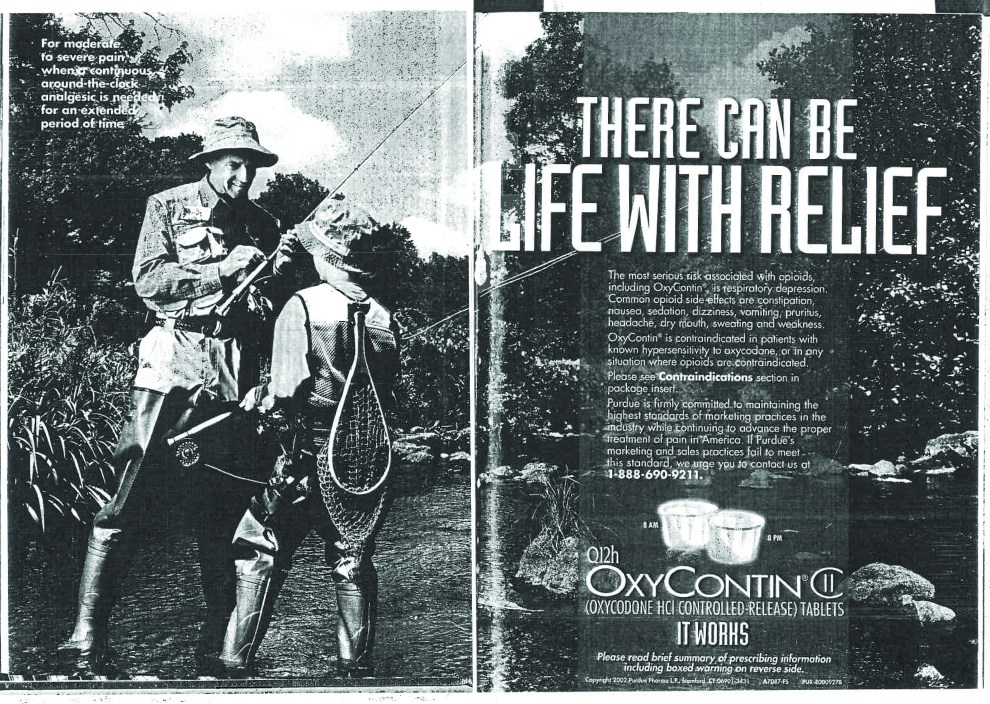
In 2002 alone, Purdue paid the organization and its foundation more than $1 million, the vast majority of which was earmarked for drug promotion, according to court records. That year, JAMA published a two-page ad for OxyContin featuring a man fly-fishing with his grandson, proclaiming, “There can be life with relief.” In a subsequent warning letter, the FDA said the ads were “especially troubling” and they “grossly misrepresent” the drug’s safety.
Purdue’s most direct influence, though, was arguably in the continuing medical education program. “As the spotlight shines on a few struggling with addictions, the AMA is determined to ensure that the plight of patients suffering in silence from chronic pain (nearly 75 million U.S. residents) is not lost,” then–AMA President Donald Palmisano wrote when he announced the program in 2003. By the end of that year, more than 84,000 physicians had already ordered the materials. (The AMA declined to share the total number of physicians who took the training.)
Funding continuing medical education, we now know, was a particularly common and insidious way that pharmaceutical companies spread pro-opioid messaging. “It’s a form of influence dressed in the clothes of legitimate medical education,” says Miriam Laugesen, a health policy researcher at Columbia University. When an organization like the AMA takes funding, she says, “they don’t see the link between continuing medical education workshops and somebody getting addicted. It’s not like they set out to do that. But in the aggregate, all of these people getting the message that these drugs were safe was really destructive, because they weren’t safe.”
The team that developed the AMA’s curriculum was also deeply intertwined with opioid makers. Among the principal faculty was Dr. Russell Portenoy, a long-time paid speaker for Purdue who argued that opioids were a “gift from nature” that were being underused due to “opiophobia” among doctors. Dr. Charles Argoff, a course adviser, received more than $600,000 from opioid manufacturers over a three-year period, a Senate report would later find. Their involvement appears to have violated the AMA’s own code of medical ethics, which suggests that “when possible, [continuing medical education] should be provided without such support or the participation of individuals who have financial interest in the educational subject matter.” (The AMA says that it adheres to “very strict rules and policies” for how industry funding is used, put forth by the Accreditation Council for Continuing Medical Education.)
Purdue’s donations to the foundation outlasted its medical training, with the company paying the philanthropic body a total of $1.5 million. More than half of Purdue’s funding to the foundation went toward supporting dozens of “prescription medication safety” programs for kids from 2011 to 2016. They ranged from a drug abuse prevention class for third and fourth graders in Marlinton, West Virginia, to a program hosting “Facebook and Twitter parties” for teens in Boise, Idaho. The grants were a good look for Purdue during a time when the company was facing increasing scrutiny from lawmakers and the general public for fueling the overdose crisis. As Laugesen notes, “Having the imprimatur of the AMA on any product or service or movement is going to help that organization sell its product.”
Beyond the optics, the grants served another purpose: They enabled Purdue executives to have access to the foundation’s Corporate Roundtable, a small group of top corporate donors—which, over the years, have included opioid makers Teva, Mallinckrodt, Allergan, and Johnson & Johnson—that met twice a year with the leadership of the AMA Foundation, and, often, the leadership of the AMA itself. In 2013 and 2017, AMA CEO James Madara met with foundation donors to speak about the AMA’s history and goals. In 2016, Patrice Harris, the longtime head of the organization’s Opioid Task Force, which leads the AMA’s opioid-related advocacy, met with corporate donors to provide an update on her group’s work. Other speakers at the foundation’s roundtable meetings have included the AMA’s director of science and biotechnology, Barry Dickinson; VP of government affairs, Cynthia Brown; and senior legislative attorney, Daniel Blaney-Koen.
The AMA contends that such meetings have no bearing on the organization’s policy. As Madara wrote to Mother Jones, “There is a bright line separating the work of the AMA from the work of the AMA Foundation.” In practice, the safeguards don’t appear to be particularly solid; at times, the leadership of the AMA and the foundation have been overlapping. In 2014, when the AMA’s Opioid Task Force launched under the leadership of Harris, she also sat on the board of the foundation, to which Purdue was a top donor. (Harris wrote in an email that her “singular purpose” in advocacy is to present AMA policy, and that her 2016 meeting with donors was a “one-sided update.”)
The AMA’s collaboration with pharmaceutical companies making opioids wasn’t limited to Purdue. In the fall of 2013, for instance, a group called the Alliance to Prevent the Abuse of Medicines launched, composed of the AMA, pharmaceutical company Teva, and a handful of other companies in the health care space. Publicly, the group claimed that drug abuse is a “national, public health crisis that must be confronted and addressed through collaborative effort.” By 2015, its members had met with members of Congress, the ONDCP, and the CDC.
But a memo produced by Teva in subsequent litigation casts the alliance’s advocacy in a different light. The alliance launched just as Teva was preparing to roll out a supposedly abuse-deterrent version of the opioid hydrocodone—and just as lawmakers were further cracking down on opioid prescribing. “Recognizing that this hostile environment will hinder the ability of Teva to properly market our current pain products as well as our pipeline AD Hydrocodone product,” reads the memo, “Teva conceived and worked behind the scenes to establish the ‘Alliance to Prevent the Abuse of Medicines.’”
The alliance appears to have dissolved in the subsequent years. Meanwhile, recent court documents allege that Teva pills were responsible for a fifth of the painkillers flooding into New York from 2006 to 2014.

A look at the AMA’s track record over its nearly 175 year history shows that the opioid crisis is the latest development in a long history of dissonance between the organization’s mission and its actions.
Founded in 1847, the AMA had just a few thousand members and a paltry budget for its first half-century of existence. That changed in the early 1900s, in part because the organization began offering a “Seal of Acceptance” to drugs, foods, and other items that met certain purity and transparency standards. Critics argued that the approval wasn’t based on particularly rigorous standards, but companies boasted about the AMA’s approval in JAMA advertisements and in their promotion more broadly. Land O’Lakes, for example, placed its emblem of AMA acceptance in glossy magazine ads for butter in the early ’30s even as it faced federal charges for selling adulterated butter and eggs. By 1948, journal subscriptions and advertising were bringing in $4.9 million in revenue. “The Seal is probably the biggest single ‘puller’ of advertising ever concocted, and in terms of investment, the Journal is far and away the most profitable publication in the world,” Harper’s Magazine concluded the following year.
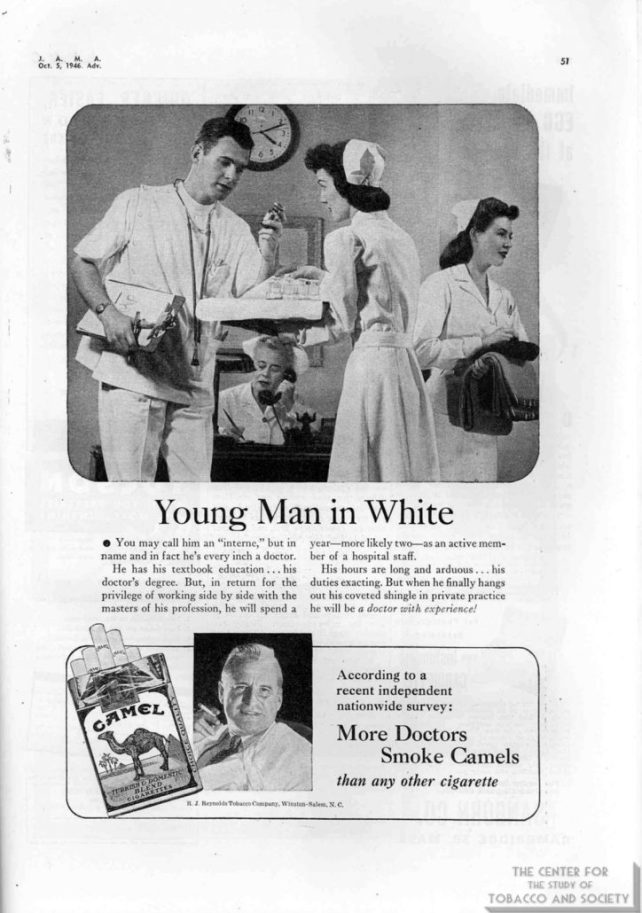
The tobacco industry also stepped in to capitalize on the AMA’s prestige. JAMA published its first cigarette advertisements in the mid-’30s, and, in the years to follow, tobacco companies became some of the journal’s largest sources of advertising revenue. The ads cleverly suggested medical approval. Camel boasted, “More doctors smoke Camels than any other cigarette,” and “Not one single case of throat irritation due to smoking Camels.” A Philip Morris ad encouraged doctors to smoke and chat in the doctors’ lounge at the 1942 AMA convention: “Stationary and stenographic services with our compliments.”
JAMA stopped running cigarette ads in the ’50s, but the AMA’s collaboration with the tobacco industry continued for decades. In 1964, after the surgeon general issued a landmark report concluding that smoking causes cancer, the Federal Trade Commission called for warning labels on cigarette packages—and ran into opposition from the AMA. “I’m really perplexed,” wrote then–FTC Commissioner Everette MacIntyre. “Thousands of doctors and many individual medical societies favor the proposed warnings, but the AMA…[says] there is no further need for educational statements to the youth. This is precisely the position of the tobacco industry.”
Instead of joining the myriad public health organizations sounding alarm bells about the dangers of smoking, the AMA in 1964 launched a sprawling research partnership with six tobacco companies. The companies gave $18 million over the next decade to the AMA’s foundation, which in turn distributed the funding to researchers for the project. Despite the big tab, in 1978, the industry-backed research effectively concluded that the surgeon general’s report was correct. But the study was successful in a more subtle way: It enabled the AMA to avoid indicting tobacco companies for years.
The AMA had good reason to stall. Many of the politicians who opposed government regulation of Big Tobacco were the same politicians who opposed government interventions in the health care system. In 1971, then–AMA Executive Director Ernest Howard was “most anxious to avoid any incident which will create displeasure with AMA among tobacco area Congressmen,” according to an internal Tobacco Institute memo issued after an institute executive met with Howard. “He said AMA needs their support urgently.”

As the AMA was working to preserve its relationship with Big Tobacco, it was also laying the groundwork for a much more lucrative future, one that would reap profits from across the medical world—from private practice physicians to large hospital systems to the federal government.
The revenues were an outgrowth of one of the organization’s most long-held positions: opposition to national health insurance. Back in the 1930s, the AMA opposed all health insurance on the grounds that “no third party must be permitted to come between the patient and his physician in any medical relation.” Later, in the 1960s, when liberals tried to establish Medicare, they faced a staunch opponent in the AMA, which warned of “socialized medicine.” In the 1980s, when Congress tried to reign in spiraling Medicare costs, the AMA’s CEO warned that doctors “are really worried that they’re not going to be allowed to practice medicine as they know it…based on their own judgment.” And while the AMA later supported the passage of the Affordable Care Act, today it continues to oppose a single-payer option.
But even as it advocated against public insurance, the AMA succeeded in taking control of a crucial part of the system. In order to pass Medicare in 1965, liberal policymakers agreed to keep the “fee-for-service” system, in which each procedure and service is billed separately, effectively incentivizing physicians and hospitals to provide more treatment. The AMA took on the job of categorizing these procedures and services into thousands of five-digit codes, called the Current Procedural Terminology. In 1983, the federal government adopted the CPT for Medicare reimbursement, and other insurers soon followed suit, according to Laugesen’s book, Fixing Medical Prices.
Today, the codes are still owned and operated by the AMA, and virtually every corner of medicine depends on them to be reimbursed for their services; when patients receive health care from doctors, physicians, labs, and hospitals bill insurance using the CPT. A cottage industry of software and billing companies has sprung up to help manage the process—and they pay the AMA to be licensed to do so. The AMA declined to specify how much revenue the CPT brings in, but more than half of the association’s total revenues—$245 million—come from “royalties and credentialing products.”
Further sweetening the deal, the AMA also heavily influences how much each code is worth—another result of the organization’s lobbying. In the ’80s, Congress commissioned a team of researchers to study how to reduce health care spending, leading to an intricate system in which each medical service was assigned a relative value based on how much time it took and how technically difficult it was to perform, among other factors. Congress adopted the system, called the Resource-Based Relative Value Scale, but it needed someone to take up the job of continually updating it. The AMA jumped on the opportunity. As Harvard economist William Hsiao, who led the researchers, explains, “They lobbied successfully with the first Bush presidency, saying, ‘The government doesn’t have to spend any money, and the government doesn’t have to interfere. You save money, you save political problems, you save your efforts, you won’t be criticized. Just let us do it.’”
Now, every year, doctors representing each specialty gather at the AMA headquarters in Chicago to go over new procedures and to haggle over their worth. The AMA then sends the proposed values to the Centers for Medicare and Medicaid Services, which, the vast majority of the time, accepts them.
A recent BMJ article put the arrangement and its impact in perspective: “With CPT, the AMA had not only found a way effectively to control government involvement in healthcare, it had also developed a way to directly profit from it,” it concludes. “This annual income has allowed the AMA lobby to maintain outsized influence over American healthcare.”
There’s yet another ubiquitous AMA-run system that drives profits: The Physician Masterfile, a database that, for more than a century, the AMA has kept of every practicing physician and their specialties, educational histories, addresses, and more. The AMA licenses health information companies to use the data—which in turn sell it to pharmaceutical companies. The data is invaluable to drug producers: By matching up the Masterfile with prescribing data collected from pharmacies, pharmaceutical companies are able to create a prescribing history for every doctor in the country and target potentially lucrative prescribers.
This is, in fact, exactly what Purdue did. The pharmaceutical giant maintained a contract with IMS Health, a market research company co-founded by Richard Sackler’s uncle Arthur. The AMA sold Physician Masterfile data to IMS Health, which, in turn, provided Purdue with detailed prescriber information. “Using this precise, AMA-enabled tracking data, Purdue was able to direct its sales effort toward high prescribers of pain medications, enabling an army of 1,000 Purdue reps, backed by a first-year marketing budget of $200 million, to descend on these soft targets,” wrote medical historian Mike Magee in his 2019 book about medical profiteering, Code Blue.
In 2006, facing multiple state bills threatening to crack down on the sharing of prescriber data, the AMA proposed a compromise: If prescribers wanted to, they could enroll in a program that would prevent their information from being shared with sales reps, though it would still be made available to pharmaceutical companies for marketing and research purposes. Even at the time, AMA leaders acknowledged that this was not simply a selfless act. In a 2006 Pharmaceutical Executive article about the new opt-out program, executives from the AMA and IMS Health called on pharmaceutical companies to regulate themselves and police their own sales forces. “If they succeed, legislators will turn their attention elsewhere, and the industry can hang onto one of its most valuable data sources,” they wrote.
Just 36,000 physicians—less than four percent—are currently enrolled in the opt-out program. Many doctors still have no idea that their information is collected, let alone sold, by the AMA, Fugh-Berman notes. (The AMA disputes this claim.) “Whenever I mention to medical students that their names are sent to the AMA when they enter medical school and tracked from that point on, they’re always outraged,” says Fugh-Berman. In 2019, the AMA’s sale of the Masterfile and other “database products” brought in nearly $60 million in revenue.
All these systems—the CPT, the Resource-Based Relative Value Scale, the Physician Masterfile—have created a steady stream of revenue even as AMA membership as a proportion of all doctors has declined over the past half-century. As of 2019, just 19 percent of practicing physicians were AMA members; nearly half of them were students or residents, who get a discount on the $420 membership fee. Membership dues currently make up just 8 percent of the AMA’s total revenue.
“They take the funds from these commercial endeavors, and then they’re able to put that into political action, like lobbying,” says Laugesen. “It’s not really an organization that your family doctor’s sending off $50 a year to protect her interests in Washington. It’s much more complicated than that. It’s much bigger.”

Today, the medical field is at war with itself: Some doctors are wary of prescribing too many painkillers, while others contend that the pendulum has swung too far in response to the opioid crisis, making it difficult for patients who need the medications to get them.
Based on how the AMA bills itself, as the unified voice of medicine, it’s reasonable to expect that the organization would play the role of medical arbiter, helping doctors and the industry more broadly navigate such complicated territory. “Most people, if they read in the paper that the AMA says this and that, they think, ‘Well, they must know.’ The assumption is that they’re a neutral source with no interest,” says Keith Humphreys, a professor of psychiatry and behavioral sciences at Stanford.
In reality, he concludes, “They’re a trade organization, but they’re not thought of that way.”
Therein lies the problem: While the AMA upholds the sacred doctor-patient relationship, its pharmaceutical funding and dependence on commercial revenue streams make it virtually impossible to discern where public health guidance ends and industry interests begin.
Over the past decade, the AMA has taken some steps to distance itself from opioid producers. “The medical profession’s understanding of opioids and the dangers associated with these drugs is different today than it was even a few years ago,” explained the AMA Foundation’s Executive Director Barkley Payne in an email. Today, the courses on pain management are free of funding from pharmaceutical companies. Payne declined to share tax filings detailing how much money the foundation receives from various donors, but said that the foundation stopped taking money from opioid makers in 2018. A year later, Purdue Pharma declared bankruptcy.
It may seem, then, that opioids are finally going the way of tobacco. The decision to stop taking opioid money came exactly 40 years after the AMA’s tobacco study concluded that smoking did, indeed, cause cancer. In both cases, the organization eventually acknowledged the dangers of a product that public health advocates had been warning about for years. In both cases, one could argue that the pronouncements came too late, after the damage was already done.
“Regardless of whether we’re talking opioids or other pharmaceutical products, it’s reasonable to question whether the AMA should be relying on funding from pharmaceutical manufacturers to do its business,” says Caleb Alexander, an epidemiology professor at Johns Hopkins. “It’s all too easy to justify these relationships based on any number of safeguards that may be put in place. Do we have a better AMA with millions of dollars of commercial funding flowing in, or would we have a better AMA without such funding? That’s an important question to deliberate and get right.”
For now, there’s little to suggest the AMA won’t repeat its mistakes if another Purdue comes along. Just last year, the AMA hosted a discussion with its new top corporate donor. It was titled “Stronger Together: A conversation with PhRMA.”
Note: This article has been updated.